presenting a new case of “Big little findings”. Radiographs belong to a 62-year-old man diagnosed of colon carcinoma one year ago. Talc pleurodesis performed after discovering right pleural implants.
Click here to see the answer
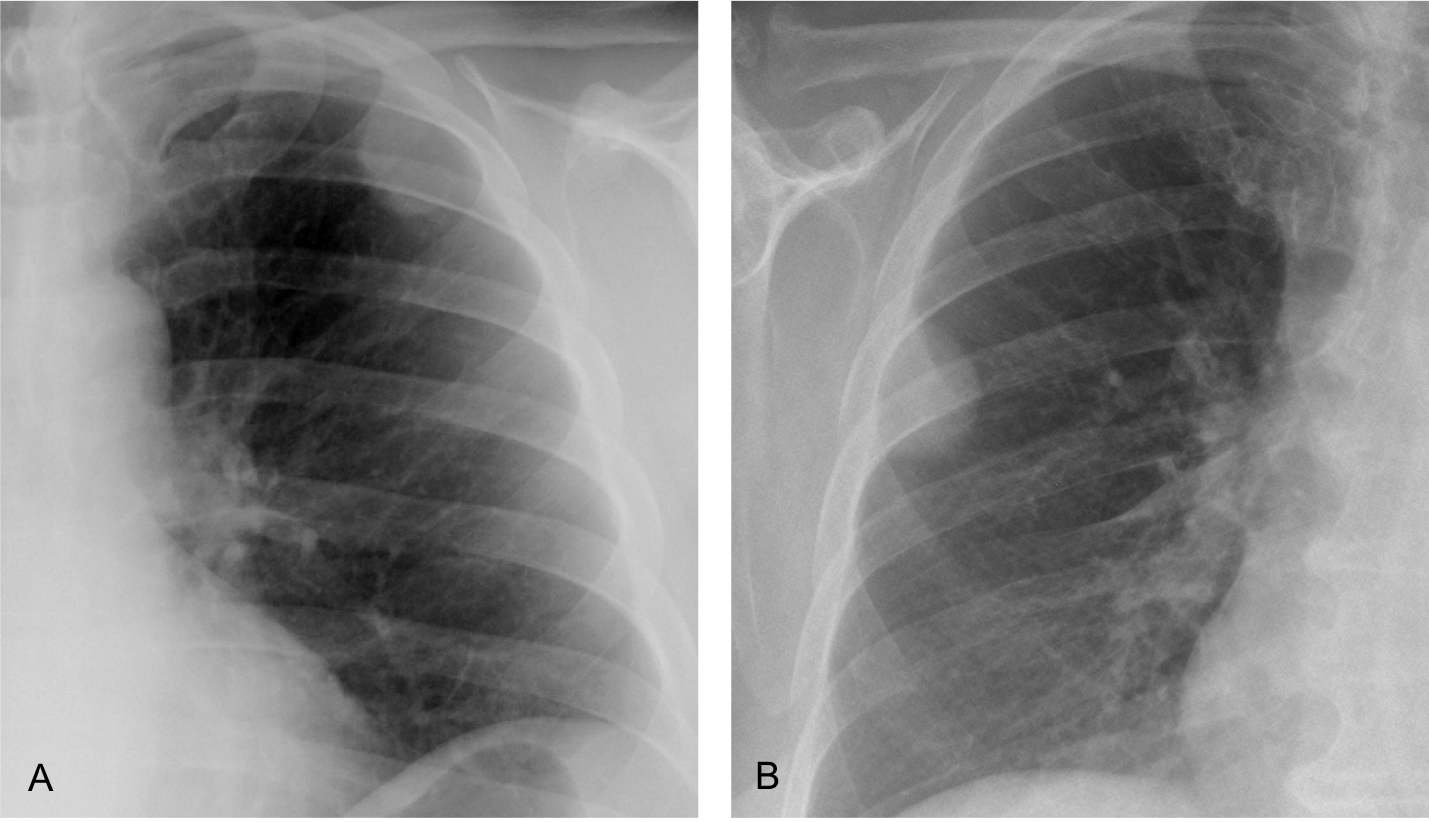
Findings: PA radiograph (A) shows a right pleural effusion, secondary to talc pleurodesis. The lateral view shows D9 loss of height with erosion of the inferior vertebral plate (B, circle). The findings are partially obscured by the superimposed pleural effusion and are better seen in the insert (C).

Comparison with a sagittal CT taken six months earlier confirms that the chest radiograph findings were not present at that time (D and E, circles).

Coronal and sagittal CT show crumbling of D9 (A and B, circles). There is air in the intervertebral space, which goes against infection. MRI confirms the findings (C and D, circles). Final opinion was metastasis vs. compression fracture. Given the lack of trauma and the presence of metastases in other organs, metastasis was considered the best diagnosis. No further action was taken.

Final diagnosis: metastasis to D9 (unproven)
I am presenting this case to emphasize, once again, the importance of looking at the thoracic spine, an important landmark in the chest radiograph. Hidden by the mediastinal structures in the PA view, it is clearly depicted in the lateral radiograph.
It is important to check the spine in each lateral view because it can offer information that may be overlooked.
This case includes three basic points to remember when reading chest radiographs:
1. Satisfaction of search. The pleural effusion centers our attention and prevents examining other areas that may show important findings.
2. Comparison with previous films. Very useful to demonstrate that the finding is real and was not present previously.
3. Performing a thorough checklist. Discovering the abnormal vertebra takes a conscious effort of analysis of the lateral view, a routine that should not be forgotten.
Once the spinal abnormality is found, cross-sectional imaging (CT and/or MRI) is the method of choice to confirm the findings and reach a likely diagnosis.
To reinforce this concept, I am showing three more cases of spinal disease that might have been missed if we had not paid attention to subtle findings.
CASE 1. 73-year-old woman with back pain for one month. Lateral chest shows a compression fracture of D12 (A, circle), partially hidden by the diaphragm. The fractured vertebra is better seen in the cone-down view (B). Compression fractures of vertebral bodies are related to osteoporosis and common in advanced age. They cause significant pain, leading to inability to perform daily activities. If they are not recognized, they lead to a decline in the well-being of elderly patients.

CASE 2. 57-year-old man with back pain. Initial film shows D9 height loss that was overlooked (A, arrow). Three months later there is obvious collapse of D9 (B, arrow). CT confirms the collapsed vertebra and irregularity of the D10 upper plate (C, circle). Diagnosis: tuberculosis

CASE 3. 34-year-old man with back pain and fever. PA chest film (not shown) was uninformative.
Lateral view shows increased opacity of the middle third of the thoracic spine and an indistinct D7-D8 space (A, circle). Findings are more evident in the cone-down view (B).

Sagittal CT shows irregularity of the intervertebral disk and erosion of the end plates (C, circle).
Coronal and axial CTs show soft-tissue involvement, responsible for the increased opacity in the lateral chest film (D and E, arrows).
Diagnosis: infectious spondylitis


Follow Dr. Pepe’s advice:
Remember to look at the thoracic spine in the lateral radiograph. You may see subtle findings that portend relevant disease.
This is the way the world ends
Not with a bang but a whimper
(T S Eliot)
Dear friends,
This is our last case. For diverse circumstances Dr. Pepe and I have decided to abandon the EBR blog. We hope you’ve enjoyed the cases and that they’ve contributed to your education. Thanks for the interest you have shown over the years.
Our best wishes to you all.