Prof. Cáceres is preparing a new webinar about the “Pulmonary fat, my friend”. Join him this Wednesday June 16th at 12:00 CEST. He will discuss the case presented here, among others. Register here.
Dear Friends,
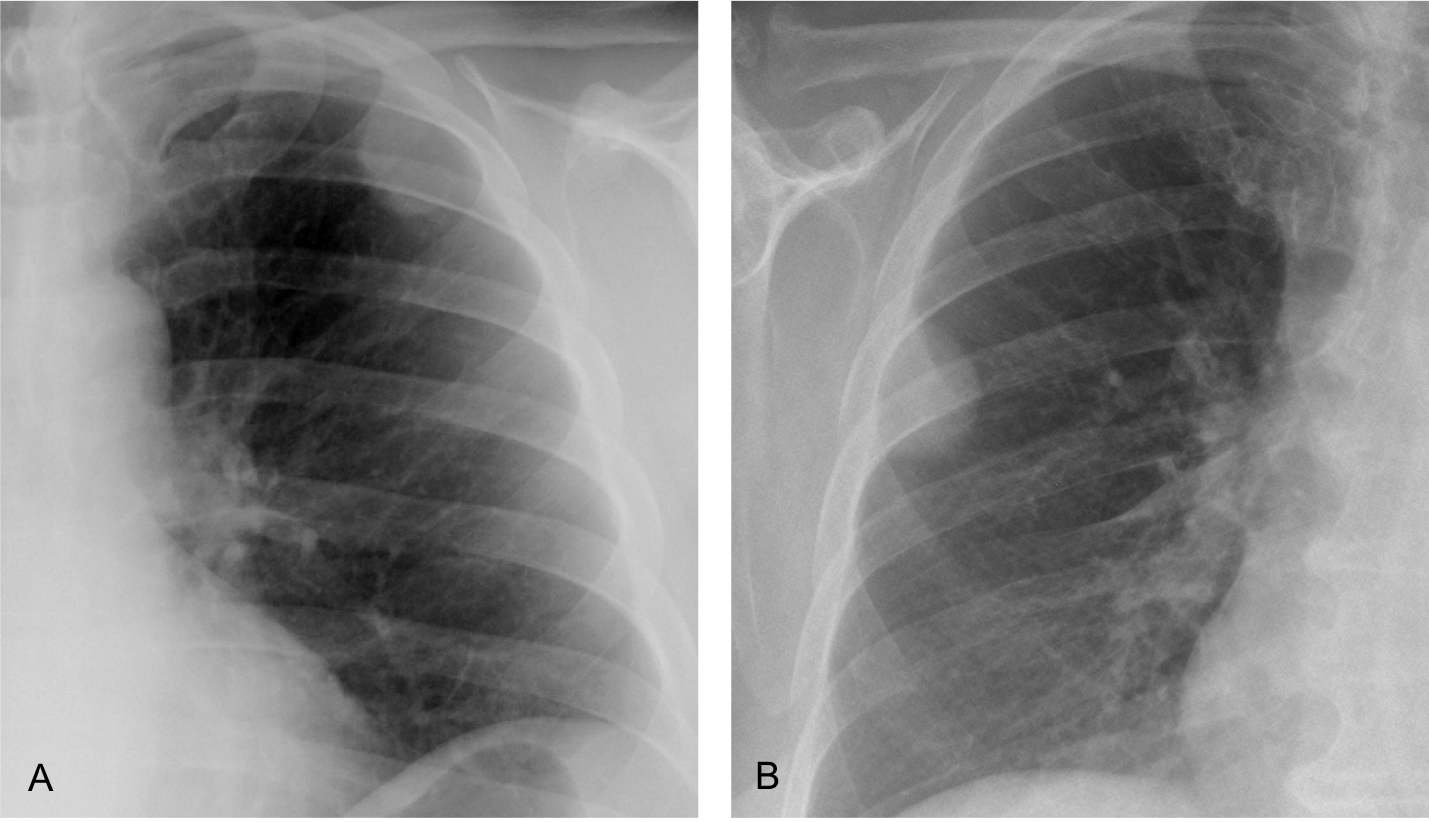
Today’s radiographs belong to two different patients with peripheral opacities of the chest. What would be your diagnosis?
1. A is fat and B solid tissue
2. B is fat and A solid tissue
3. Both are fatty
4. Need a CT
Click here to see the answer
Findings: Radiograph of case A shows an opacity in the left upper lung. Its inner contour is outlined by air (arrow) and the outer border is not visible (asterisk) suggesting an extrapulmonary lesion (incomplete border sign).
CT shows that the opacity represents extrapleural fat (B, arrow).
Radiograph of the second case shows a well-defined rounded opacity (C, arrow), that was interpreted as a peripheral pulmonary nodule. PET-CT was done, and the apparent pulmonary nodule was shown to be extrapleural fat (D, arrow).
These two cases are shown to emphasize that fat in or around the lung cannot be distinguished from soft tissues in the plain chest radiograph. To recognize fat, CT is necessary.
More information about fatty lesions of the lung is given in the webinar “Mediastinal fat: my friend” that will be published soon on the EBR youtube channel.
presenting a new case of “Big little findings”. Radiographs belong to a 62-year-old man diagnosed of colon carcinoma one year ago. Talc pleurodesis performed after discovering right pleural implants.
What do you see?
Click here to see the answer
Findings: PA radiograph (A) shows a right pleural effusion, secondary to talc pleurodesis. The lateral view shows D9 loss of height with erosion of the inferior vertebral plate (B, circle). The findings are partially obscured by the superimposed pleural effusion and are better seen in the insert (C).
Comparison with a sagittal CT taken six months earlier confirms that the chest radiograph findings were not present at that time (D and E, circles).
Coronal and sagittal CT show crumbling of D9 (A and B, circles). There is air in the intervertebral space, which goes against infection. MRI confirms the findings (C and D, circles). Final opinion was metastasis vs. compression fracture. Given the lack of trauma and the presence of metastases in other organs, metastasis was considered the best diagnosis. No further action was taken.
Final diagnosis: metastasis to D9 (unproven)
I am presenting this case to emphasize, once again, the importance of looking at the thoracic spine, an important landmark in the chest radiograph. Hidden by the mediastinal structures in the PA view, it is clearly depicted in the lateral radiograph.
It is important to check the spine in each lateral view because it can offer information that may be overlooked.
This case includes three basic points to remember when reading chest radiographs:
1. Satisfaction of search. The pleural effusion centers our attention and prevents examining other areas that may show important findings.
2. Comparison with previous films. Very useful to demonstrate that the finding is real and was not present previously.
3. Performing a thorough checklist. Discovering the abnormal vertebra takes a conscious effort of analysis of the lateral view, a routine that should not be forgotten.
Once the spinal abnormality is found, cross-sectional imaging (CT and/or MRI) is the method of choice to confirm the findings and reach a likely diagnosis.
To reinforce this concept, I am showing three more cases of spinal disease that might have been missed if we had not paid attention to subtle findings.
CASE 1. 73-year-old woman with back pain for one month. Lateral chest shows a compression fracture of D12 (A, circle), partially hidden by the diaphragm. The fractured vertebra is better seen in the cone-down view (B). Compression fractures of vertebral bodies are related to osteoporosis and common in advanced age. They cause significant pain, leading to inability to perform daily activities. If they are not recognized, they lead to a decline in the well-being of elderly patients.
CASE 2. 57-year-old man with back pain. Initial film shows D9 height loss that was overlooked (A, arrow). Three months later there is obvious collapse of D9 (B, arrow). CT confirms the collapsed vertebra and irregularity of the D10 upper plate (C, circle). Diagnosis: tuberculosis
CASE 3. 34-year-old man with back pain and fever. PA chest film (not shown) was uninformative.
Lateral view shows increased opacity of the middle third of the thoracic spine and an indistinct D7-D8 space (A, circle). Findings are more evident in the cone-down view (B).
Sagittal CT shows irregularity of the intervertebral disk and erosion of the end plates (C, circle).
Coronal and axial CTs show soft-tissue involvement, responsible for the increased opacity in the lateral chest film (D and E, arrows).
Diagnosis: infectious spondylitis
Follow Dr. Pepe’s advice:
Remember to look at the thoracic spine in the lateral radiograph. You may see subtle findings that portend relevant disease.
This is the way the world ends
Not with a bang but a whimper
(T S Eliot)
Dear friends,
This is our last case. For diverse circumstances Dr. Pepe and I have decided to abandon the EBR blog. We hope you’ve enjoyed the cases and that they’ve contributed to your education. Thanks for the interest you have shown over the years.
Our best wishes to you all.
This week’s case follows the pattern of a “Meet the Examiner” presentation, with questions and answers similar to a real examination. Take your time before scrolling down for the answer.
There will be no new blog posts over the Easter period. The next case will be published on Monday, April 5, 2021.
The images belong to a 65-year-old woman with cough and low-grade fever. The referred physician demanded a chest CT.
What would be your diagnosis?
1. Pneumonia
2. Pulmonary infarction
3. Peripheral adenocarcinoma
4. Any of the above
Click here to see the answer
Findings: unenhanced axial and sagittal CTs show LLL airspace disease with a surrounding halo (B-C arrows). In my opinion, the sensible answer is 4. Any of the above, although I liked adenocarcinoma because of the peripheral halo and air bubbles within the infiltrate (A, circle).
Click here to see more images
Patient was diagnosed of pneumonia and treated with antibiotics, without improvement. Chest radiographs taken 13 days later shows progression of the LLL opacity (A and B, arrows).
A CT was recommended.
Click here to see the CT images
Two axial and one sagittal views are selected. What would your diagnosis be:
1. Peripheral adenocarcinoma
2. Tuberculosis
3. Covid pneumonia
4. None of the above
Click here to see the answer
In comparison with the previous CT, the LLL infiltrate has increased markedly in less than two weeks. An upper halo persists (A and C, arrows). A small infiltrate has appeared at the right lung base (B, arrow) In my opinion, this rapid progression rules out carcinoma and TB. A PCR was negative. Blood tests were not remarkable. It was considered that the patient had an unusual pneumonia, and the antibiotic was changed.
Click here to see more images
The fever disappeared with the new antibiotic and the patient improved moderately. A new CT was taken three weeks later. What would your diagnosis be?
1. Löffler syndrome
2. Goodpasture syndrome
3. Cryptogenic organizing pneumonia
4. Any of the above
Click here to see the answer
Findings: The most striking finding is the disappearance of the LLL infiltrate and the apparition of two new areas of airspace disease in RLL and LLL (A, arrows). There is a halo sign in the LUL infiltrate (B, arrows) and a negative halo in the RLL infiltrate (B and C, arrows).
This change of location of the opacities falls in the category of migratory infiltrates which are caused by several diseases, some of them listed in the previous questions.
The patient had no risk factors for parasitic infection and no peripheral eosinophilia, ruling out Löffler syndrome. Renal function was not altered, excluding Goodpasture’s syndrome
The combination of migratory infiltrates and a negative halo sign was very suggestive of a cryptogenetic organizing pneumonia, that was confirmed with BAL and an excellent response to corticosteroid treatment.
Final diagnosis: cryptogenic organizing pneumonia
Organizing pneumonia (OP) is a clinical, radiological and histological entity usually associated to other pathologies. The idiopathic form of OP is called cryptogenic organizing pneumonia (COP).
Clinical manifestations of COP begin with a mild flu-like illness with fever, cough and malaise.
In chest imaging it may appear as localized airspace opacity that may be confused with ordinary pneumonia, adenocarcinoma or aspiration, among others. The lack of response to antibiotic treatment and the peripheral location may help in suggesting the diagnosis.
I am presenting this case because it shows two features the help in the diagnosis: migratory infiltrates and the reverse halo sign.
Migratory infiltrates are not unique to COP, but they occur in a limited number of diseases (Loeffler syndrome, vasculitis, etc.) and their presence in the adequate clinical setting should suggest COP.
The reverse halo was originally described as specific of COP, but since then it has been seen in many other entities. It is defined as a central ground-glass opacity surrounded by denser consolidation of crescentic shape or a complete ring. It is visible in about 20% of cases.
In this patient the combination of both signs strongly pointed towards COP, that was confirmed and responded brilliantly to corticoid treatment.
To complete the presentation, I am showing two more examples of reversed halo and migratory infiltrates (CASES 1 and 2, below).
CASE 1. 61-year-old woman with COP and basilar infiltrates (A, arrows). During treatment, coronal and axial CTs show bilateral and symmetrical reversed halo signs (B and C, arrows)
CASE 2. 51-year-old woman with COP and migratory pulmonary infiltrates (A and B). The second CT shows nice examples of reversed halo sign (B, circle), better seen in the cone down axial view (C, arrows).
Follow Dr. Pepe’s advice:
1. Localized cryptogenic organizing pneumonia may mimic other pulmonary processes
2. Migrating infiltrates and reverse halo sign (or both) are helpful in suspecting COP
Presenting a new case of “Big little findings”. Preoperative chest radiograph for meniscus surgery in a 56-year-old woman.
What do you see?
Click here to see the answer
Findings: PA view shows a small right hemithorax. There is elevation of the right hemidiaphragm and a small hilum (A, red arrow). The findings are very suggestive of RLL lobectomy. The oblique fissure in the RLL represents the displaced minor fissure (A, white arrow). Previous CT shows a normal-size right lung with a ground-glass opacity in the RLL (B, arrow).
Final diagnosis: RLL lobectomy for adenocarcinoma of the lung
I am showing this case to discuss displacement of the lung fissures, an important finding that can indicate partial collapse of the underlying lobe. Usually, lobar collapse is detected because of the increased opacity of the lobe. Occasionally, the collapsed lobe retains much of its air, so a shift of the fissure may be the only sign of collapse.
A potential pitfall of fissure displacement is previous surgery, as seen in the case presented. In my experience, excluding previous surgery, aerated lobar collapse occurs mainly in the following conditions:
NORMAL ANATOMY
The right minor fissure is visible in about 50% of chest radiographs as a straight horizontal line at the level of the right hilum (Fig. 1, A and B) The right and left major fissures are not visible in the PA film because their course is not tangential to the x-ray beam. (A, curved dotted lines). They are both visible as oblique lines in the lateral view (B).
Fig. 1Fig. 2. PA radiograph showing the minor fissure (A, arrow). The lateral view shows both the right minor and major fissures (B, white arrows) and the upper portion of the left major fissure (B, red arrow)
Inflammatory lesions can cause scarring which diminishes the size of the affected lobe. TB is the most common cause in upper lobes. Bronchiectasis is the predominant cause in lower lobes. Both conditions can show an aerated lobe with loss of volume (Figs. 3-5).
Fig. 3. 68-year-old woman with previous history of TB. There is aerated partial collapse of RUL as evidenced by the elevated minor fissure (A and B, white arrows). Fibrotic changes are seen in the apex (A and B, red arrows). An incidental finding is calcification of breast prostheses.Fig. 4. RLL collapse secondary to bronchiectasis. There is an oblique line at the right base (A, white arrow) that simulates an inferior accessory fissure. However, the right hilum is markedly low (A, red arrow), indicating loss of volume of RLL. Coronal CT shows marked RLL collapse with bronchiectasis, outlined by the displaced major fissure (B, arrow).Fig. 5. 56-year-old man with previous TB. Lateral view shows forward displacement of the left major fissure (A, arrows), indicating partial collapse of LUL. PA radiograph depicts marked elevation of left hilum (B, arrow), secondary to fibrotic TB.
Central lobar bronchial obstruction is occasionally associated with aerated lobar collapse. It is thought to be due to collateral air ventilation through incomplete fissures (Figs. 6-7).
Fig. 6. Routine follow-up of an 82 y.o. man who underwent surgery for laryngeal carcinoma 10 years ago. PA view shows abnormal left hilum and blurring of the left cardiac contour (A, arrow). Lateral view shows marked forward displacement of the left major fissure (B, arrows) indicating severe LUL collapse.
Unenhanced axial CT confirms the marked LUL collapse (C, white arrow) secondary to endobronchial obstruction (C, red arrow). CT taken one year earlier shows an endobronchial lesion (D, red arrow) and discrete forward displacement of the major fissure (D,E, white arrows). These changes were overlooked. Surgical diagnosis: bronchogenic carcinoma
Fig. 8. Aerated RLL collapse in central carcinoma. PA radiographs shows a very low right major fissure (A, red arrow), better depicted in the cone down view (B, arrow). The left hilum is descended (A, white arrow). Bronchoscopy discovered a carcinoma of the RLL bronchus. The oblique line in the RUL corresponds to a scar.
Rounded atelectasis is a common cause of fissure displacement. It occurs secondary to spiral folding of the lung parenchyma when fixed by thickened pleura. The consequence is a peripheral rounded opacity in an aerated collapsed lobe. The volume loss, detected by the displaced fissure, avoids possible confusion with a true nodule in the plain film.
Fig. 9. Asymptomatic 49-year-old man with rounded atelectasis. Notice the visibility of the left major fissure, indicating LLL volume loss (A, arrows). Lateral view shows an ill-defined posterior opacity which corresponds to the rounded atelectasis (B, arrow).
Axial and sagittal CT confirm displacement of the left major fissure (C and D, white arrows), the small LLL, and the posterior rounded atelectasis (C, red arrow).
As a final thought, occasionally you may find fissure displacement without an apparent cause (Fig. 10).
Fig. 10. 92-year-old man, asymptomatic. PA radiograph shows downward displacement of the minor fissure (A, white arrow), major fissure (A, yellow arrow) and right hilum (A, red arrow). In a previous film four years earlier, the minor fissure (B, yellow arrow) and the right hilum (B, red arrow) were moderately descended. Since the patient was 92 y.o. and had no symptoms, his physician decided not to do a CT scan. My impression is that he has fibrotic changes in the RLL, which is not unusual in advanced age.
Follow Dr. Pepe’s advice:
1. A displaced fissure may be the only manifestation of aerated lobar collapse (always exclude previous surgery).
This week’s case is a little special! Prof. Cáceres has prepared a Quiz that will to challenge your knowledge and your speed reviewing radiographs! The quiz contains 7 different cases with radiographs and you will have 60 seconds to answer each question! The three participants with highest score will receive a signed picture of Dr. Pepe 😀
Are you up for the challenge? Join the quiz here It will start on Thursday 18th, at 12:00 CET.
On Friday Prof. Cáceres will publish the explanation for each case on the blog.
CASE 1
CASE 1
71-year-old man with hemoptysis:
In which quadrant will you place the lesion?
1. Right upper quadrant
2. Right lower quadrant
3. Left upper quadrant
4. Left lower quadrant
Click here to see the answer
Findings: there is a rounded opacity behind the heart (A, arrow). CTs show a non-enhancing pulmonary mass with irregular borders attached to the pericardium (B-C, circles).
Post-operative diagnosis: mucoid carcinoma of the lung.
CASE 2
CASE 2
43-year-o.ld male with moderate cough.
Most likely diagnosis:
1. Tuberculosis
2. Enlarged left pulmonary artery
3. Carcinoma
4. Any of the above
Click here to see the answer
Findings: PA radiograph shows that the left hilum is larger and more opaque than the right one (A, arrow). The pulmonary arch is prominent (A, red arrow). The lateral view shows an enlarged left pulmonary artery (B, arrows) excluding the diagnosis of carcinoma or TB as causes of hilar enlargement. Enhanced axial CT confirms the enlarged left pulmonary artery (insert, arrow).
Diagnosis: Congenital pulmonary valve stenosis with secondary dilatation of the left pulmonary artery due to the jet effect.
CASE 3
CASE 3
60-year-old man with chest pain.
In which quadrant will you place the lesion?
1. Right upper quadrant
2. Right lower quadrant
3. Left upper quadrant
4. Left lower quadrant
Click here to see the answer
Findings: there is a well-defined rounded left apical opacity (A, arrow), better seen in the cone down view (B, arrow)
Coronal and axial enhanced CT confirm the apical mass (C-D, arrows). The patient complained of pain in the left shoulder. Needle biopsy came back as adenocarcinoma.
Final diagnosis: Pancoast tumor
CASE 4
CASE 4
65-year-old man with cough and dyspnea
Diagnosis:
1. Unilateral hyperlucent lung
2. Pneumothorax
3. Giant bulla
4. Carcinoma of the lung
Click here to see the answer
Findings: the initial impression of the PA chest is a left hyperlucent lung with diminished vascularity. A second look shows a descended left hilum (A, arrow) and a concave paraspinal line (A, red arrow) representing the major fissure. These findings are indicative of LLL collapse with compensatory expansion of LUL.
Enhanced axial CT confirms the marked LLL collapse (B, arrow). Coronal reconstruction shows irregular bronchial narrowing (C, red arrow) with complete occlusion of the LLL bronchus.
Diagnosis: epidermoid carcinoma with LLL collapse.
CASE 5
CASE 5
33-year-old man with pain in the right hemithorax
Where is the nodule located:
1. Lung
2. Pleura
3. Chest wall
4. Need a CT
Click here to see the answer
Findings: PA radiograph shows a rounded opacity in the lower right chest (A, circle) with incomplete border sign (medial aspect outlined by air, lateral border not visible because in contact with chest wall). The clue to its location is given by the rib erosion (A, red arrow) which places the lesion in the underside of the rib. The border of the erosion is sclerotic, indicating a slow-growing process.
CT confirms a soft-tissue mass (B, circle) and the rib erosion (B-C, red arrows).
Final diagnosis: neurofibroma in a patient with neurofibromatosis.
CASE 6
CASE 6
32-year-old man with chronic cough
In which quadrant will you place the lesion?
1. Right upper quadrant
2. Right lower quadrant
3. Left upper quadrant
4. Left tower quadrant
Click here to see the answer
Findings: PA radiograph shows increased lucency of the lower right lung with decreased vasculature (A, circle). This finding has two main causes: increased lung air or paucity of lung vessels (pulmonary embolism, arterial stenosis). In these cases, the best approach is to take an expiratory film, which will demonstrate whether or not there is air-trapping. If present, it will orient us to a bronchial obstructive process, either central or peripheral
Coronal CT (B) confirms the increased lucency and diminished vasculature of RLL and RML. Scattered bronchiectasis are seen within the lucent lung (B-C, arrows).
Axial expiratory CT (D) demonstrates marked air-trapping of RML and RLL.
The patient had a history of swallowing a peanut at the age of five years, developing RLL pneumonia at that time. Control radiographs demonstrated increased lucency of the lower right lung over the years.
Final diagnosis: Lobar Swyer-James/McLeod syndrome secondary to aspiration of a peanut in childhood.
Findings: PA radiograph shows a rounded opacity in the periphery of the left lung (A, arrow) that seems to be calcified. Cone down view shows a whorled pattern (B, arrow). A braid is visible in the left supraclavicular area (A, red arrow).
Scout view of the CT does not show the apparent lung lesion, which is not visible in the axial view of the lung (D). The technician that did the CT noticed that the patient had a long braid with a rubber band at the end.
Final diagnosis: hair braid simulating a lung nodule.
Dear friends,
Presenting today a new case of “Big little findings”. This case is not recommended for the faint-hearted 😱
Chest images belong to a 65-year-old woman with moderate cough. Since I am your friend, I am including an axial CT.
What do you think?
Click here to see the answer
Findings: PA radiograph shows a curvilinear opacity in the right middle/lower lung (A, arrows). The right lung is slightly smaller than the left and the hilum looks abnormal (A, circle). Aside from slight elevation of the right hemidiaphragm, the lateral view (B) is unremarkable.
Coronal CT shows that the curvilinear line represents a scimitar vein draining below the diaphragm (C, arrow). The right pulmonary artery describes an unusual path (D, circle) and there is abnormal branching of the right main bronchus (D, circle).
An unexpected finding is an oblique band in the lower right lung (E and F, arrows). The bronchi and RLL vessels pass through an opening in the center (E and F, circles).
Final diagnosis: hypogenetic right lung with duplicated diaphragm
The reason I’m presenting this case is to discuss duplication of the diaphragm, an uncommon congenital malformation associated with hypogenetic lung.
As you all know, hypogenetic lung is a congenital malformation characterized by absence of one or two lobes of the right lung, with abnormal lower lung venous drainage (scimitar vein) in 80% of cases. It is asymptomatic and almost always occurs on the right side. Because it is symptomless, it is usually found incidentally in adults .
Typical signs in the PA chest radiograph (Fig. 1) reflect the small size of the lung:
1. Small right hemithorax with secondary dextrocardia
2. Small right hilum
3. Anomalous vein in RLL (scimitar sign), not always present
Fig. 1. PA radiograph (A) shows typical appearance of hypogenetic lung: small right hemithorax, secondary dextrocardia, and a scimitar vein (A, arrows) coursing downwards to join the IVC. Enhanced coronal CT in a different patient shows the scimitar vein to better advantage (B, arrow). Axial CT confirms the small right hemithorax and abnormal branching of the right main bronchus (insert, circle).
Occasionally, hypogenetic lung occurs with minimal hypoplasia, a normal-sized right lung, and absent dextrocardia. In these patients (such as the initial one), the scimitar vein and abnormal right hilum are the clues to the diagnosis.
In my experience, these cases are the ones most commonly associated with duplicated diaphragm, an infrequent malformation resulting from an alteration of caudal migration of the embryonic diaphragm.
Anatomically it appears as a band running obliquely from the chest wall to the right hemidiaphragm (Fig. 3, drawing).
If we’re lucky, we might see it as an oblique line in PA and lateral radiographs (Fig. 4), but it is usually not visible or overlooked (Fig. 5). An additional sign is blurring of the central part of the right hemidiaphragm, where the duplication ends (Figs. 4 and 5).
Fig. 3. Coronal and axial drawings demonstrating the appearance of the duplicated diaphragm (A and B, blue lines) and vessels crossing through the central orifice (A and B, in red).Fig. 4. Duplicated diaphragm visible in the PA and lateral radiographs as an oblique band (A and B, white arrows). Note that the contour of the right hemidiaphragm becomes blurred where the duplicate joins it (A and B, red arrows). Axial CT confirms the duplicated diaphragm (C, white arrows) and crossing vessels (C, red arrow). A scimitar vein was not present in this patient.Fig. 5. Blurring of the central right hemidiaphragm (A, red arrow) and an oblique line in the lateral view (B, red arrow) were present in the initial case, but they were overlooked. Signs in the chest radiograph can be too subtle. My advice is to rely on the CT findings.
My hard-learned experience tells me it is very difficult to suspect duplicated diaphragm on plain films. It is usually discovered in a CT performed to confirm a hypogenetic right lung or for other reasons.
The good news is that the CT findings are pathognomonic and consist of:
1. An oblique band with a central opening
2. RLL bronchi and vessels passing through the opening and fanning out thereafter
You may wonder why I present such a rare condition, but the answer is simple:
a) It is easily recognized because of the distinctive findings. Once recognized, advise against surgery or other invasive procedures.
b) I don’t believe it’s that rare. In my career I have seen a dozen cases, the last three in this century and at the same institution. The last, seen in 2015, is the one that headed this Diploma. Two more were seen in 2004 and 2008 (Cases 1 and 2, below).
I am due to see a new case soon. Perhaps in a COVID patient, allowing me to write a useless paper about the relationship between COVID and duplicated diaphragm 🙂
CASE 1. 56-year-old woman investigated for lymphoproliferative syndrome. Axial and coronal CT show an unsuspected duplicated diaphragm (A and B, white arrows) and the crossing vessels (A and B, red arrows).CASE 2. CT requested for chronic bronchitis in a 44-year-old woman. Axial CTs document the complete duplicated diaphragm (red arrows), the vessels insinuating through it (B, circle) and lower down, the orifice with the vessels passing through (C, green arrow). White arrows point to the downward course of the scimitar vein before draining in the IVC.
Follow Dr. Pepe’s advice:
1. Duplicated diaphragm is an infrequent malformation associated with hypogenetic right lung
2. Difficult to detect in the chest radiograph
3. Easy to diagnose in CT images by the following signs:
a) Oblique band with a central hiatus in the right lower lung
b) Central hiatus that constricts RLL bronchi and vessels
I am starting a new section named “Big little findings”. The aim is to emphasize the importance of discovering subtle findings that should not be missed. They are easily seen if you know what to look for.
Today I’m showing preoperative chest radiographs of a 69-year-old man with bladder carcinoma.
What do you see?
Click here to see the answer
Findings: the most important feature is a negative finding: absence of air in the gastric fornix (A, circle). Although this is sometimes seen in healthy persons, it is more frequent in distal esophageal obstruction. A careful look discovers that the left mediastinum has a double contour, actually the left wall of the dilated esophagus (A, blue arrow) and the descending aorta (A, red arrow). There is bulging of the right paraesophageal line (A, yellow arrow). A dilated air-filled upper esophagus is visible in the lateral view (B, arrows).
The findings are typical of lower esophageal obstruction with dilatation of the esophagus. The double contour of the left mediastinum is better seen in the cone down view (C, arrows) and confirmed with CT (D, arrows).
The air-filled dilated esophagus in the lateral view (E, arrows) is confirmed with sagittal CT (F, arrows) (T= trachea).
Final diagnosis: unsuspected esophageal achalasia
To my eternal shame, I confess that when I read the initial radiographs I overlooked the findings (nobody’s perfect!). Achalasia was discovered in a routine follow-up CT taken one year later. I redeemed myself in a subsequent pre-op PA radiograph of the patient, in which I saw a double contour of the descending aorta (A and B, red and blue arrows) and bulging of the paraesophageal line (A and B, yellow arrows). I missed the absent air in the gastric fornix, again!
Esophageal achalasia is not an uncommon condition, and early stages can be suspected in the chest radiograph if we pay attention to the telltale signs. Note that these signs are not specific for achalasia and can be secondary to any obstructive process of the distal esophagus. The most revealing findings are:
Absent gastric bubble
Displaced lower mediastinal lines
Air-fluid level in the mediastinum
ABSENT GASTRIC BUBBLE
Occurs in about 10% of the normal population and 50% of achalasia patients, and is due to failure of swallowed air to cross the distal esophageal sphincter. It is a negative finding and therefore, difficult to recognize. When it is detected, we should examine the lower mediastinum, looking for signs of esophageal dilatation (Fig. 1).
Fig. 1. 54-year-old man with moderate dysphagia. In the PA radiograph, there is no gastric bubble (do not confuse air in the colon – A and B, black arrows – with air in the gastric fornix). The paraesophageal line is convex (A, red arrow). These two signs are suspicious for achalasia, confirmed with barium swallow. Note the distal esophageal stenosis (B, white arrow).
DISPLACED LOWER MEDIASTINAL LINES
A dilated esophagus displaces the paraesophageal line toward the right, making it convex. The left wall of the esophagus moves outward, and is sometimes seen as a double contour with the descending aorta (Figs. 2 and 3). Convexity of the paraesophageal line is the most reliable sign and the easiest to detect.
Fig. 2. 48-year-old. woman with achalasia. Initial film shows a normal mediastinum with a visible gastric bubble (A, black arrow). Four years later (B) the gastric bubble is absent. There is a second contour (B, red arrow), paralleling the aorta (B, black arrow). Note that the initial concave paraesophageal line has become straight four years later (A and B, yellow arrows). Esophagogram confirms the esophageal dilatation and the narrow esophagogastric junction (C, red arrow). Fig. 3. 47-year-old man with dysphagia. PA radiograph shows a convex paraesophageal line (A, white arrow). There is also a convex line on the left (A, red arrow). CT confirms the dilated esophagus containing air and fluid (B and C, asterisks). Diagnosis: esophageal achalasia.
AIR-FLUID LEVEL IN MEDIASTINUM
Excluding hiatal hernia, an air-fluid level in the mediastinum is usually located in the esophagus. It is seen as a straight horizontal line in the middle/upper mediastinum. It is usually related to esophageal obstruction of any cause, the most common being achalasia. Discovery of an air-fluid level should lead us to investigate other signs of esophageal dilatation (Figs. 4 and 5).
Fig. 4. 47-year-old woman with dysphagia. PA radiograph shows an air-fluid level in the upper mediastinum (A, red arrow) accompanied by bulging of the paraesophageal line (A, white arrow) and absent gastric fornix. Esophagogram: dilated esophagus with distal stenosis (B, arrow) typical of achalasia. Fig. 5. Showing this case because it’s a beauty. 73-year-old man referred by the pulmonologist to investigate chronic cough. PA and lateral chest radiographs show a dilated esophagus containing mainly air (A and B, white arrows), with a distal air-fluid level (A and B red arrows). Axial CT confirms the dilated esophagus with retained food (Insert, arrow). Achalasia, confirmed. Air is visible in the gastric fornix in this case (A, black arrow).
Aspiration pneumonia is a complication of achalasia. I’m showing two cases in which the signs mentioned helped to suggest the correct diagnosis (Figs. 6 and 7).
CASE 1.
55-year-old man with pancreatic carcinoma and known achalasia who presented with marked cough. Chest radiographs show bilateral airspace infiltrates. In the PA view there is also dilatation of the upper esophagus (A, white arrows) with an air-fluid level (A, red arrow). The lateral view shows a retrocardiac mass (B, white arrow), suggestive of a dilated lower esophagus. The trachea is displaced forward (B, red arrow). These signs were overlooked by the radiologist, whose diagnosis was widespread pneumonia.
Coronal CT demonstrates widespread air-space disease. It also shows a dilated esophagus (C, arrow). Axial CT images confirm dilatation of the esophagus, which is full of residue
(D and E, arrows).
Final diagnosis: esophageal achalasia with secondary aspiration pneumonia.
CASE 2.
This an old case of a 27-year-old woman with a chronic RUL opacity suspected to be TB (disregard the opacities in both middle lung fields, caused by superimposed breast implants).
PA chest radiograph shows an opacity in the right upper lobe (A, circle). A right paramediastinal line extends from top to bottom (A, arrows). The lateral view shows anterior displacement of the trachea by a tubular structure (B, arrows), which occupies the upper and middle mediastinum. Both findings suggest a dilated esophagus.
Barium swallow confirms the dilated esophagus, secondary to narrowing at the esophagogastric junction (insert, arrow). Considering the age of the patient, achalasia with aspiration pneumonia was the most likely diagnosis, confirmed later.
(Remember that aspiration pneumonia goes to the right upper lobe when the patient is recumbent at night).
Follow Dr. Pepe’s advice:
Subtle findings of distal esophageal obstruction (achalasia) that should not be overlooked:
showing today a preoperative AP chest of a 93-year-old man who broke his right femur after a fall.
What do you see?
Click here to see the answer
Findings: AP chest radiograph shows a poorly defined opacity in the RUL (A, circle).
Axial and coronal enhanced CT show that the opacity corresponds to a tortuous brachiocephalic artery (B and C, arrow). There is no pulmonary infiltrate.
Final diagnosis: Tortuous brachiocephalic artery simulating a pulmonary infiltrate.
The aim of this Diploma is to continue discussing chest imaging in the older population.
Today I will comment about the main manifestations of aging in the mediastinum and heart, discussing variants that may simulate disease, followed by the most common conditions affecting these regions in elderly patients.
NORMAL VARIANTS
The standard PA radiograph in aging adults usually shows a somewhat enlarged mediastinum, due to poor inspiratory effort combined with an elongated aorta and mediastinal fat accumulation (Fig. 1) .
Fig. 1. Normal chest in an 85-year-old man. Note the limited inspiration and increased width of mediastinum. The aorta is elongated, and the cardiothoracic ratio is 50%. A pacemaker is visible in the left hemithorax.
A common variant in older patients is a tortuous brachiocephalic artery, which may project into the lung, simulating a pulmonary lesion (Fig. 2), as was shown in the initial case.
Fig. 2. 88-year-old woman with vague chest complaints. PA radiograph shows an RUL opacity (A, circle). Unenhanced axial CT confirms that the opacity corresponds to a tortuous brachiocephalic trunk projecting into the lung (B, arrow).
Sometimes the tortuous artery simulates a mediastinal mass. In these cases, the diagnosis is easy because a mediastinal mass pushes the trachea toward the left (Fig. 3A), whereas an elongated artery does not; instead, the associated elongated aorta displaces the trachea to the right (Fig. 3B).
Fig. 3. 52-year-old man with a right thyroid mass pushing the trachea towards the left (A, arrow). The second patient is an 83-year-old man with tortuous brachiocephalic vessels simulating a mediastinal mass (B, arrow). Note that the trachea is displaced towards the right by an elongated aorta.
The aorta is elongated in most older adults. A kink in the distal descending aorta often casts a posterior shadow in the lateral view that should not be confused with disease (Fig. 4).
Fig. 4. 73-year-old man with an elongated aorta (A). A kink in the descending aorta creates a posterior opacity superimposed on the lower spine (B, circle). Unenhanced sagittal CT confirms the kink as the cause of the opacity (insert, arrow).
Calcification of the annulus fibrosus of the mitral valve is common in elderly individuals. It does not cause symptoms and should not be confused with other conditions. It has a pathognomonic appearance in the chest radiographs (Fig. 5).
Fig. 5. 79-year-old man/woman with mitral annulus calcification. Note the typical “C” shape and location in the PA and lateral radiographs (A and B, circles).
A variant of calcified annulus fibrosus is a condition termed caseous necrosis of the mitral annulus. It appears as an ovoid intracardiac calcification, visible in chest radiographs (Fig. 6) and confirmed with CT. It is also symptomless.
Fig. 6. 73-year-old man, asymptomatic. PA and lateral radiographs demonstrate an ovoid calcification projected over the cardiac shadow (A and B, arrows). Axial CT confirms the calcification (insert, arrow), corresponding to caseous necrosis of the annulus.
PATHOLOGY
The most common mediastinal pathology in the older population is hiatus hernia, easily identifiable when it contains air. An airless hernia should not be confused with a lower mediastinal mass. The best way to diagnose hiatus hernia is by looking at previous films (Fig. 7). If none are available, a barium swallow is sufficient (Fig. 8).
Fig. 7. 68-year-old woman with an airless hiatus hernia simulating a mediastinal mass (A, arrow). Previous film one year earlier shows a typical hernia with an air-fluid level (B, arrow).Fig. 8. PA and lateral radiographs in a 65-year-old woman with a large airless hiatus hernia (A and B, arrows) . No previous films. Barium swallow confirms the hernia (insert, arrow).
At times, too much air in a hernia may be misleading, as occurred in the case below, which was initially diagnosed as a possible pneumopericardium (Fig. 9).
Fig. 9. 66-year-old woman with known breast carcinoma admitted to the ER in shock. AP radiograph show right lung metastasis (A, arrow) and two lines outlined by air surrounding the heart (A, red arrows).
Pneumopericardium was suspected. Enhanced CT coronal and sagittal images
show that the apparent pneumopericardium was actually a large hiatus hernia (B and C, arrows). On retrospective review of the patient’s chest radiograph, bowel air can be seen projected over the heart.
Mediastinal mass in patients of advanced age are commonly due to metastasis. Lymphoma is an alternative diagnosis, as around 50% of non-Hodgkin lymphomas occur in patients older than 65 years (Fig. 10).
Fig. 10. 77-year-old woman with asthenia and weight loss. Chest radiographs show bilateral pleural effusion and an anterior mediastinal mass (A, arrows. B, asterisk). Axial CT confirms the mass (insert, arrow). Diagnosis: B-cell lymphoma
Differentiating aortic aneurysm from a tortuous aorta is difficult in chest radiographs, because the medial aortic wall is obscured by the mediastinum. Sometimes the inner wall is outlined by air, allowing detection of aortic dilation in the plain film (Fig. 11).
Fig. 11. 73-year-old woman with chest pain and a tortuous aorta. The medial wall is outlined by air, allowing us to determine that the aorta is dilated (lines in A and B). Enhanced axial CT shows a type-B aortic dissection (insert, arrow).
The incidence of atrial fibrillation increases after the age of 65, and up to 9% of octogenarians are affected with this condition. Detecting a prominent left atrium in the chest radiograph of an elderly person should suggest this diagnosis (Fig. 12).
Fig. 12. 75-year-old woman with atrial fibrillation. Note the prominent left atrium in the PA and lateral radiographs (A and B, arrows).
Ventricular aneurysm is a complication of myocardial infarction. In an elderly patient, the aneurysm may calcify and appear as curvilinear calcium projected over the left heart (Fig. 13).
Fig. 13. 80-year-old man with a history of myocardial infarction ten years earlier. Chest radiographs show a thin curvilinear line projected over the heart, consistent with a calcified aneurysm (A and B, arrows). Unenhanced CT confirms the diagnosis (insert, white arrows). A calcified thrombus is also visible (insert, red arrow).
Follow Dr. Pepe’s advice:
1. Tortuous brachiocephalic artery and calcification of the mitral annulus are common variants in persons of advanced age.
2. Hiatus hernia occurs frequently in older individuals.
3. Enlarged left atrium in this age group should raise the possibility of atrial fibrillation.
This is the last case on 2020 and we will be back on January 11, 2021!
Today I will show a new “Meet the examiner case”, with questions and answers similar to a real presentation. You will get more images on Wednesday and the final answer on Friday.
Images belong to a 49-year-old woman with progressive chest pain and dyspnea. She mentions being hit in the chest with a surfboard three weeks ago.
Diagnosis:
1. Myocardiopathy
2. Pericarditis
3. Myelolipoma
4. Any of the above
What do you see?
Click here to see more images
Cardiac ultrasound discovered a large pericardial effusion that was drained, evacuating a large amount of hematic fluid (A)
Three days days later the patient developed mild symptoms of cardiac tamponade. Portable chest (B) shows increased size of the cardiac silhouette. Enhanced axial CT (C) is shown.
What do you think?
Click here to see the answer
Findings: PA and lateral radiographs (A-B) show what appears to be an enlarged cardiac silhouette. Of the offered options I would think first of pericardial effusion because the pulmonary vessels are small compared to the size of the heart. In cardiomyopathy I would expect engorged pulmonary vessels. Cannot exclude thymolypoma, but I would consider it very unlikely. Probably the best answer is 4. All of the above. And I would recommend a cardiac US because traumatic pericardial effusion is the most likely diagnosis.
Cardiac ultrasound discovered a large pericardial effusion that was drained, evacuating a large amount of hematic fluid. Note the normal thickness of the pericardium (C-D, arrows)
CT also discovered healing fractures of the anterior 4th, 6th and 7th left ribs (E-G, arrows)
After drainage, the heart shadow returned to normal size (H). Three days later the patient developed fever and mild symptoms of cardiac tamponade. Portable chest showed increased size of the cardiac silhouette, despite the presence of a draining catheter (H-I, red arrows).
Enhanced CT demonstrated a moderate amount of pericardial fluid (J-K, arrows) accompanied by bilateral pleural effusions (J, red arrows). The pericardium was surgically explored and cleaned. Staphylococcus Xilosus was grown.
After appropriate antibiotic treatment the symptoms subsided. One month later the chest at discharge appeared normal (L-M).
Final diagnosis: delayed traumatic pericarditis with subsequent infection
Pericardial effusion has many causes, one of them blunt trauma. It is usually associated with other findings: pneumothorax, fractured ribs and lung contusion. Delayed pericardial effusion is a rare manifestation of previous blunt trauma.
Plain film signs of pericardial fluid are unreliable, except for visualization of posterior displacement of epicardial fat in the lateral view, which has high value (epicardial fat sign, Fig. 1). Cardiac ultrasound is the diagnostic technique of choice.
I am showing this case because of the beauty of the initial images and the iatrogenic infectious complication, which muddled the differential diagnosis.
To complete the presentation I am showing a very rare case of cardiac volvulus. It occurred secondary to surgical trauma, after removal of part of the right pericardium (Fig. 2).
I borrowed this case from an American friend a long time ago and am ashamed to confess that I don’t remember who he was. The credit is yours, friend. Many thanks.
Fig. 1. 46-year-old man with liver cirrhosis and pericardial effusion. PA radiograph(A) shows non-specific enlargement of the cardiac silhouette. The lateral view shows posterior displacement of the epicardial fat (B, arrow). The thickened pericardium is visible between the epicardial and mediastinal fat (B, red arrows).
Coronal and sagittal CT confirm the presence of a moderate amount of pericardial fluid (C-D, arrows). Note the displaced epicardial fat in the lateral view (B, red arrow).
Fig 2. 34-year-old woman with Down syndrome with chronic respiratory infections in RLL (A). Bronchoscopy discovered a hemangioma obstructing the intermediary bronchus. At surgery the tumor was adherent to the right pericardium. Pneumonectomy and partial resection of right pericardium were performed.
Post-op portable chest shows moderate prominence of the right heart border (B, arrow).
Six hours after the intervention the patient started to deteriorate and went into shock. Portable radiograph shows displacement of the cardiac silhouette to the right (C, arrow) and complete herniation of the heart into the right hemithorax twelve hours later. (D, arrow). A second intervention confirmed a cardiac volvulus that was corrected with a pericardial patch.
Follow Dr. Pepe’s advice:
1. Delayed pericarditis after blunt trauma is rare. Should be considered when the cardiac silhouette enlarges following blunt chest trauma
2. Echocardiography is the diagnostic method of choice for diagnosing pericardial fluid
3. Plain film signs of pericardial effusion are unreliable, except for visible displaced epicardial fat in the lateral radiograph
Dear Friends,
I am back with a new Diploma case. Miss Piggy sends her regards😍 and has helped to choose the case.
Chest radiographs belong to a 74-year-old man with a cough and pain in the chest.
What do you see?
Click here to see the answer
Findings: PA radiograph shows a bulge in the left paraspinal line (A, arrow), suggestive of a posterior mediastinal mass. A rounded posterior opacity is seen in the lateral view (B, arrow).
Unenhanced coronal and sagittal CT show large osteophytes displacing the paraspinal line (C, circle) pushing the aorta forward in the sagittal view(D, circle). Incidental gas is visible in the intervertebral disk.
Final diagnosis: large osteophytes simulating a pulmonary/mediastinal mass
The aim of this Diploma is to discuss chest imaging in the elderly. As patients get older the appearance of their chest radiographs changes in comparison with young persons. I intend to discuss changes associated to aging as well as the most common pathologies in the old.
I have divided the presentation into three separate chapters:
1- Bony structures of the chest
2- Heart and mediastinum
3- Lungs and diaphragm
Today I will comment on the main manifestations of aging in the chest skeleton, discussing variations that may simulate disease, followed by the most common bone pathologies in the elderly.
NORMAL VARIANTS IN THE AGED
Degenerative changes are the hallmark of the aging skeleton.Vertebral osteophytes are common and large ones should not be confused with pulmonary nodules (Fig 1) or mediastinal masses (Fig 2), as shown in the initial case. The diagnosis is easily made with chest CT.
Fig 1. 67-year-old male without significant symptoms. PA radiograph (A) is unremarkable. Lateral view shows a posterior nodule that could be intrapulmonary (B, arrow). Coronal and sagittal unenhanced CT show that the nodule represents a large osteophyte (C-D, arrows). The absence of other osteophytes makes it difficult to suspect this diagnosis in the plain film.Fig 2. 65-year-old man in whom a posterior mediastinal mass was discovered (A-B. arrows). The mass was unchanged in comparison with a previous examination. CT was recommended because a neurogenic tumor could not be excluded.Unenhanced coronal and sagittal CT demonstrates that the mass represents a single large osteophyte (C-D, arrows)
Calcification of the first costal cartilage may happen in the young but it is more common in the elderly. When asymmetrical, it may be confused with a pulmonary nodule (Fig 3). Exuberant cartilage calcification may simulate an upper lobe infiltrate (Fig 4).
Fig 3. 70-year-old man with a large pleural effusion, suspected to be malignant because of a possible nodule in the LUL (A, arrow). Cone down view shows that the nodule es calcified and corresponds to the first costal cartilage (B, arrow). Post-pneumonic empyema.Fig 4. 69-year-old woman with fever. Exuberant calcification of the first right costal cartilage was initially diagnosed as pneumonia (A, circle). Comparison with a radiograph taken four years earlier did not show any change (B-C, arrows).
Aging causes brittle bones and explains the increased incidence of costal fractures in the elderly. The callus of a healed fracture should not be confused with a pulmonary nodule (Fig. 6).
Fig 6. 74-year-old woman in whom a RUL nodule appeared one year after cardiac surgery (A, arrow). A 3-D reconstruction shows that the nodule represents a healed fracture of the second rib (B, circle). Ribs fractures after cardiac surgery are not uncommon
Resuscitation maneuvers, not uncommon in advanced age, may cause bilateral rib fractures, that should be recognized as such (fig 7).
Fig 7. 63-year-old man with prostate carcinoma, complaining of chest pain. PA radiograph shows sclerotic areas in the lower ribs (A, arrows), not present in previous films. My initial impression was metastatic disease, until I learned that the patient has had resuscitation maneuvers a few months earlier. Axial and coronal CT confirms symmetrical healed fractures of the anterior lower ribs (B-C, circles).
SKELETAL PATHOLOGY
The most common bone pathology in the elderly are fractures. Acute rib fractures are common, most of them secondary to falls (Fig 8). Detection is important because they cause respiratory impairment that may end in pneumonia with the subsequent increase of morbidity and mortality.
Fig 8. 78-year-old alcoholic man after a fall. PA radiograph shows displaced rib fractures (A, circle) as well as pneumothorax (A, red arrow) and subcutaneous emphysema Note the straight air-fluid level of hemothorax at the left base (A, arrow)
Compression fractures of vertebral bodies are related to osteoporosis and common in the elderly. They cause significant pain, leading to inability to perform daily activities. If they are not recognized they cause a decline of the quality of life in elderly patients (Fig 9).
Fig 9. 84-year-old woman with chronic back pain. PA radiograph (A) is unremarkable. Lateral chest shows a severe compression fracture of D9 (B, circle), better seen in the cone down view (C, arrows).
Lytic bone lesions in the elderly are usually related to metastases or multiple myeloma. Sclerotic metastases are common in old males. Given the prevalence of prostate carcinoma this should be our first diagnostic consideration in widespread sclerotic lesions (Fig 10). The differential diagnosis includes myelofibrosis (fig 11) and chronic renal failure (Fig 12).
Fig 10. 71-year-old male with widespread sclerotic lesions of ribs and spine secondary to metastases from prostatic carcinoma.
Myelofibrosis is a myeloproliferative neoplasm which cause osteosclerosis. The association of an enlarged spleen should alert us to this possible diagnosis.
Fig 11. Preoperatory chest film in a 67-year-old woman. Diffuse increased bone density (A), better seen in the cone down view of left shoulder (B). The medially displaced gastric bubble suggests splenic enlargement (A, arrow). Myelofibrosis suspected and confirmed.Fig 12. 73-year-old woman with chronic renal failure. PA radiograph (A) shows deformity of the rib cage. Lateral view (B) show the rugged-jersey spine, typical of this entity.
Solitary sclerotic lesions of the skeleton raises the possibility of metastasis vs. Paget disease. In the spine, Paget disease usually increases the size of the vertebra whereas metastases do not (Fig 13). In the peripheral skeleton the increase in width of the cortical bone is characteristic of Paget disease (Figs 14-15) .
Fig 13. 68-year-old man who presented with back pain. PA radiograph (A) is unremarkable. Lateral view shows an ivory vertebra (B, circle) that has the same size than the others. Diagnosis: metastasis from prostatic carcinoma.Fig 14. Two patients with Paget disease of a rib. Note the increased cortical thickness of the 6th rib in the first patient compared to the other ribs (A, arrow) a hallmark of Paget disease. The second patient has sclerosis of the whole 6th rib which is increased in size (B, arrow), another characteristic of Paget.Fig 15. 70-year-old man with prostate carcinoma and metastasis to the anterior third rib (A-B, arrows). Note the difference with the previous cases.
Follow Dr. Pepe’s advice:
1. Osteophytes and healed rib fractures may simulate pulmonary nodules in the elderly
2. It is important to detect rib or vertebral fractures in the elderly because they may be the source of complications
3. Sclerotic bone lesions in the elderly are usually due to prostate metastases or Paget disease